Coronary artery anomalies (CAAs) include several congenital conditions characterized by abnormal origin or course of any of the 3 main epicardial coronary arteries.
Type of anomaly
1. Anomalies of origin
1) Anomalous pulmonary origin of the coronaries
2) Anomalous aortic origin of the coronaries
3) Congenital atresia of the letf main artery
2. Anomalies of course
1) Myocardial (or coronary) bridging
2) Coronary aneurysm
3. Anomalies of termination
1) Coronary arteriovenous fistula
2) Coronary stenosis
Normal anatomy of the coronary arteries.


Anomalous Origin of Left Coronary Arterial Branches from Right Sinus of Valsalva

Anomalous origin of the right coronary artery from the left sinus of Valsalva

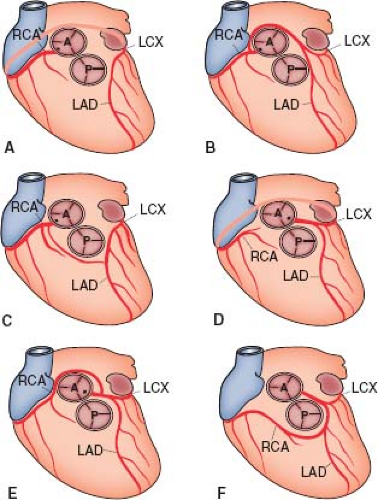
Single coronary artery variants

A 44-year-old man presented to the emergency room for typical chest pain, with nonspecific electrocardiographic abnormalities and normal high-sensitivity troponin T levels. An exercise ECG was performed and was positive for ischemic electrocardiographic changes at peak exercise and during recovery. The invasive coronary angiography showed no significant coronary stenosis; instead, an unexpected abnormality was observed: The LAD originated from the right aortic sinus, sharing the same ostium with the RCA, and the LCx emerged from the right aortic sinus but from a separate and higher ostium. CCTA showed a subpulmonic and a retroaortic course of the LAD and LCx, respectively. A stress cardiac magnetic resonance (CMR) demonstrated diffuse subendocardial inducible ischemia not matching any specific coronary supplied territory. The patient was treated conservatively.

A 42-year-old man with sudden onset of oppressive chest pain and an ECG pattern diagnostic for inferior ST-segment–elevation myocardial infarction (STEMI) was referred to our catheterization laboratory for emergency percutaneous coronary intervention. No coronary occlusion or stenoses were found, but the RCA had an abnormal origin from the left aortic sinus. At CCTA, the RCA had an initial interarterial course, with a slight lumen reduction that was more evident during systole. Over the next days, the patient remained stable, with complete resolution of symptoms and ECG abnormalities, whereas high-sensitivity troponin T progressively decreased to normal levels from a peak value of 1696 ng/L. Finally, CMR was performed to assess the presence and extent of myocardial necrosis but rather revealed morphological findings suggestive of acute myocarditis. D1 indicates first diagonal branch; LGE, late gadolinium enhancement; LMCA, left main coronary artery; LSV, left sinus of Valsalva; and RSV, right sinus of Valsalva.
Imaging and functional tests to diagnose coronary artery anomalies (CAAs) and assess myocardial ischemia.

CAAs are most often identified as unexpected findings at echocardiography or at invasive coronary angiography (ICA) or coronary computed tomography angiography (CCTA) during the diagnostic workup of ischemic heart disease. First-level functional tests (ie, exercise ECG, stress echocardiography, or nuclear imaging) may then be proposed to assess the presence of CAA-related myocardial ischemia. However, second-level tests (such as hybrid imaging, including CCTA and single-photon emission computed tomography [SPECT], or stress cardiac magnetic resonance [CMR]) may be more accurate in this clinical context by establishing the potential matching between the CAA and the ischemic territories.
https://www.ahajournals.org/doi/10.1161/circulationaha.121.055347
https://thoracickey.com/congenital-anomalies-of-the-coronary-vessels-and-the-aortic-root/
'Cardiology' 카테고리의 다른 글
| PFO (난원공 개존증, Patent Foramen Ovale) (2) | 2024.12.10 |
|---|---|
| 심신증후군 Cardiorenal syndrome (0) | 2024.11.08 |
| 관상동맥 CT 조영술 (coronary CT angiography, CCTA) (0) | 2024.07.29 |
| DCMP - 확장성 심근병증 (0) | 2024.06.17 |
| ICD 삽입형 제세동기 (0) | 2024.03.11 |



